Adverse events should be reported. Reporting forms and information can be found at www.yellowcard.mhra.gov.uk or search for MHRA Yellow Card in the Google Play or Apple App Store. Adverse events should also be reported to Nova Laboratories Ltd, Martin House, Gloucester Crescent, Wigston, Leicester, LE18 4YL Email: qa@novalabs.co.uk










Why use a liquid formulation?
As children grow older, the way in which their bodies react to medicines and dosages varies.(8)
Child appropriate formulations must be able to adapt to these changes to provide children with safe and effective dosages.(8)
Oral liquids are considered the most appropriate formulation for young children and are the preferred choice for parents and healthcare professionals.(9)
Tablet splitting is associated with potential exposure of parents/carers to cytotoxic contamination.(6)
Liquid formulations provide maximal dosing flexibility making it possible to use over a wide age range(8)
Adherence
Maximising mercaptopurine adherence and maintaining steady thiopurine exposure minimises relapses in children with ALL.(10)
Adherence to a medicine is related to many factors, but palatability and acceptability of formulations are considered key factors for children.(11)
Non-adherence, or drug interruptions, can result in relapse and emergence of resistance. 59% of relapses can be attributed to non-adherence(12)
Results of a study based on 22 participants aged 3 to 16 years(7)
How easy is it to take Xaluprine® daily?
Easy all of the time – 82%
Easy most of the time – 9%
Easy sometimes – 9%
Not easy at all – 0%
What do you think about the taste?
OK to good – 77%
Not OK to bad – 23%
What do you think about the smell?
OK to good – 91%
Not OK to bad – 9%
Offers a flexible, individualised dosing alternative to mercaptopurine tablets
- The mercaptopurine content (mg) was assayed in ten randomly selected tablet quarters*
- Two out of ten (20%) tablet quarters demonstrated >20% deviation from target 12.5 mg dose
- Two out of ten (20%) tablet quarters demonstrated >10% deviation from target 12.5 mg dose
- Drug content variation in quartered tablets shown to be attributable to weight variation during the splitting process
*Tested in-house
Tablets lack accuracy and flexibility in dosing
Quartered tablets: deviation from target 12.5 mg mercaptopurine dose
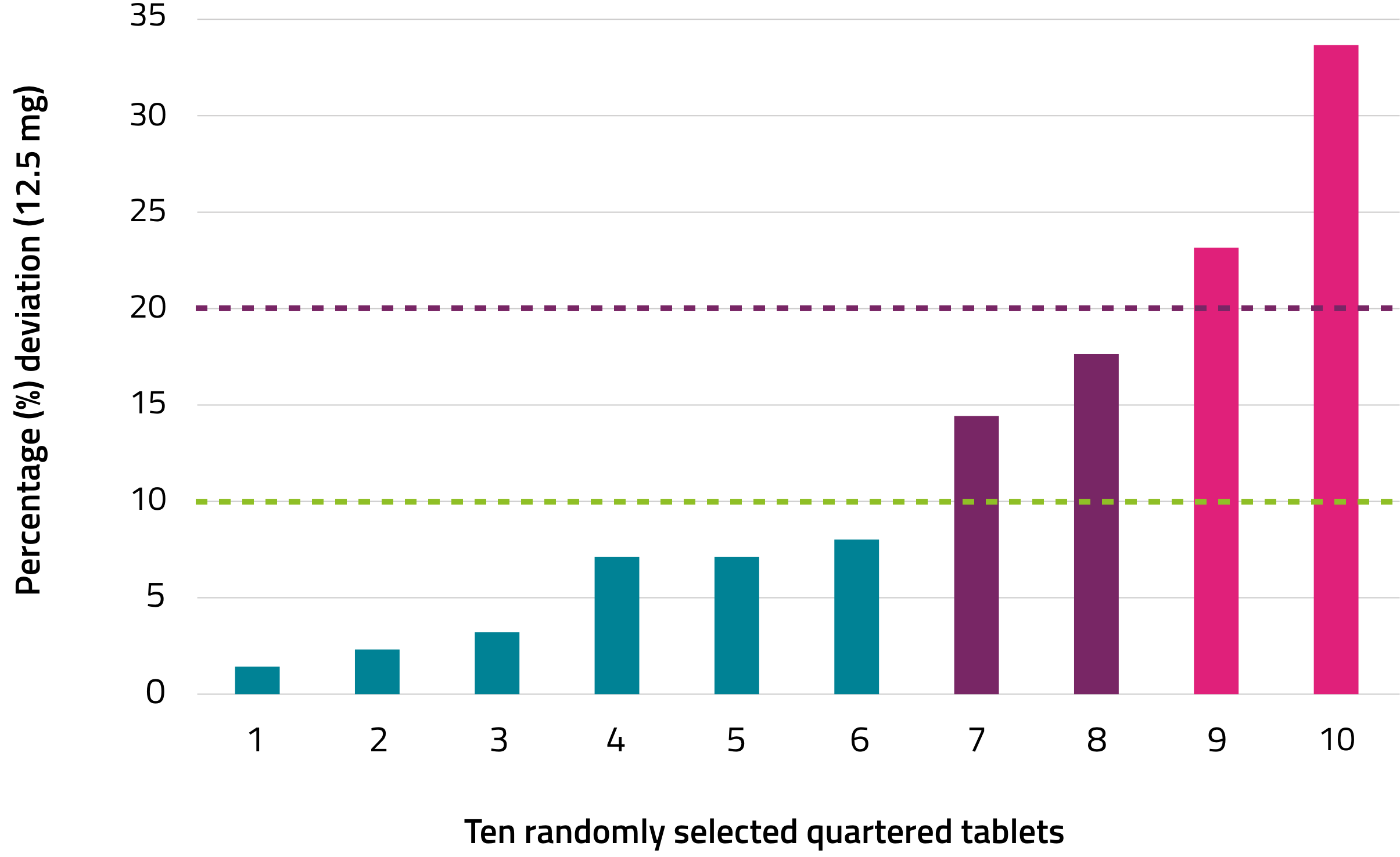
<10% deviation
>10% deviation
>20% deviation
Mercaptopurine
Mercaptopurine belongs to a group of medicines called cytotoxics (also called chemotherapy). Cytotoxics work by stopping cancer cells from multiplying.(13)
6-Mercaptopurine (6-MP), a structural analogue of guanine, has been widely used since the early 1950s as therapy for children with ALL(13)

6-MP goes under three major transformation routes, one anabolic and two catabolic, in which its intracellular activation by hypoxanthine-guanine phosphoribosyl transferase (HGPRT) forms 6-thioinosine monophosphate (TIMP).(13)
Metabolism of TIMP into 6-thioguanine triphosphate (6-TGTP) leads to its incorporation into DNA, causing miscoding during DNA replication and triggering programmed cell death. TIMP also inhibits de novo synthesis of purine which promotes incorporation of 6-TGTP into DNA.(13)
Mercaptopurine is an established treatment and a part of an established maintenance regimen for ALL patients, and is essential for patient survival.(14)
Survival rates (event-free survival) increase with the duration of mercaptopurine administration in maintenance therapy.(15)
How to use Xaluprine®
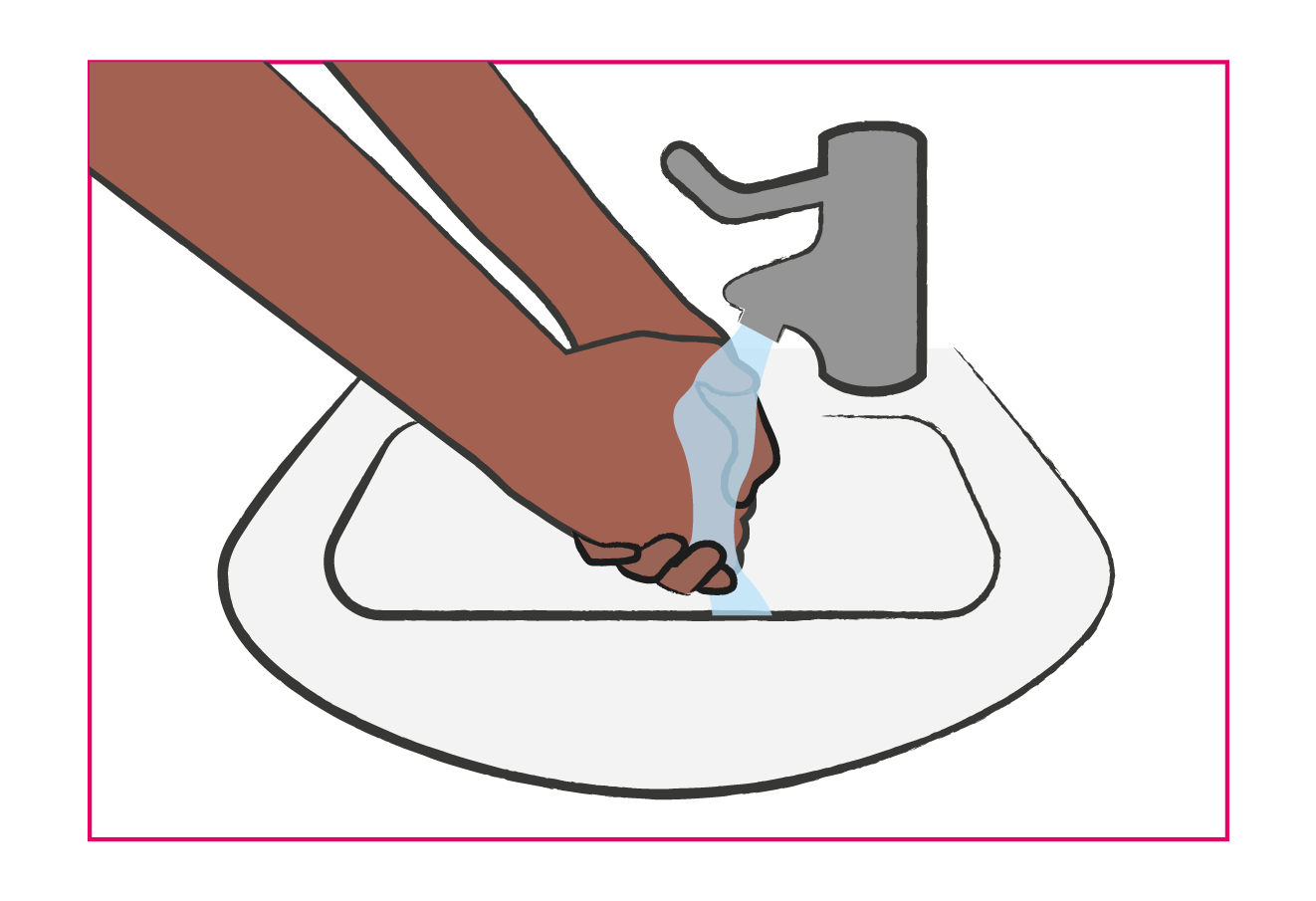
Wash your hands before and after administering a dose. Wipe up spillages immediately
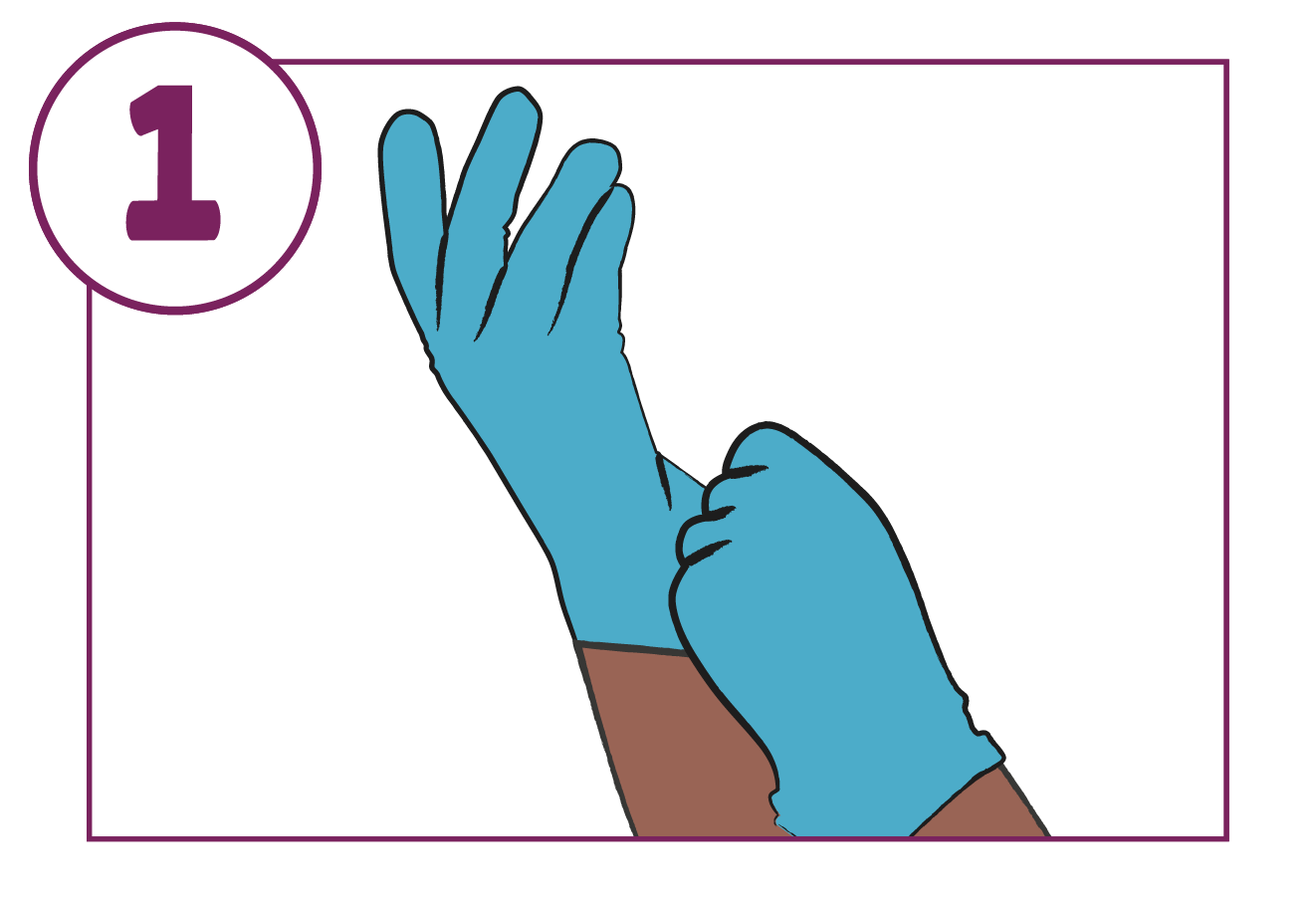
Put on disposable gloves before handling the medicine
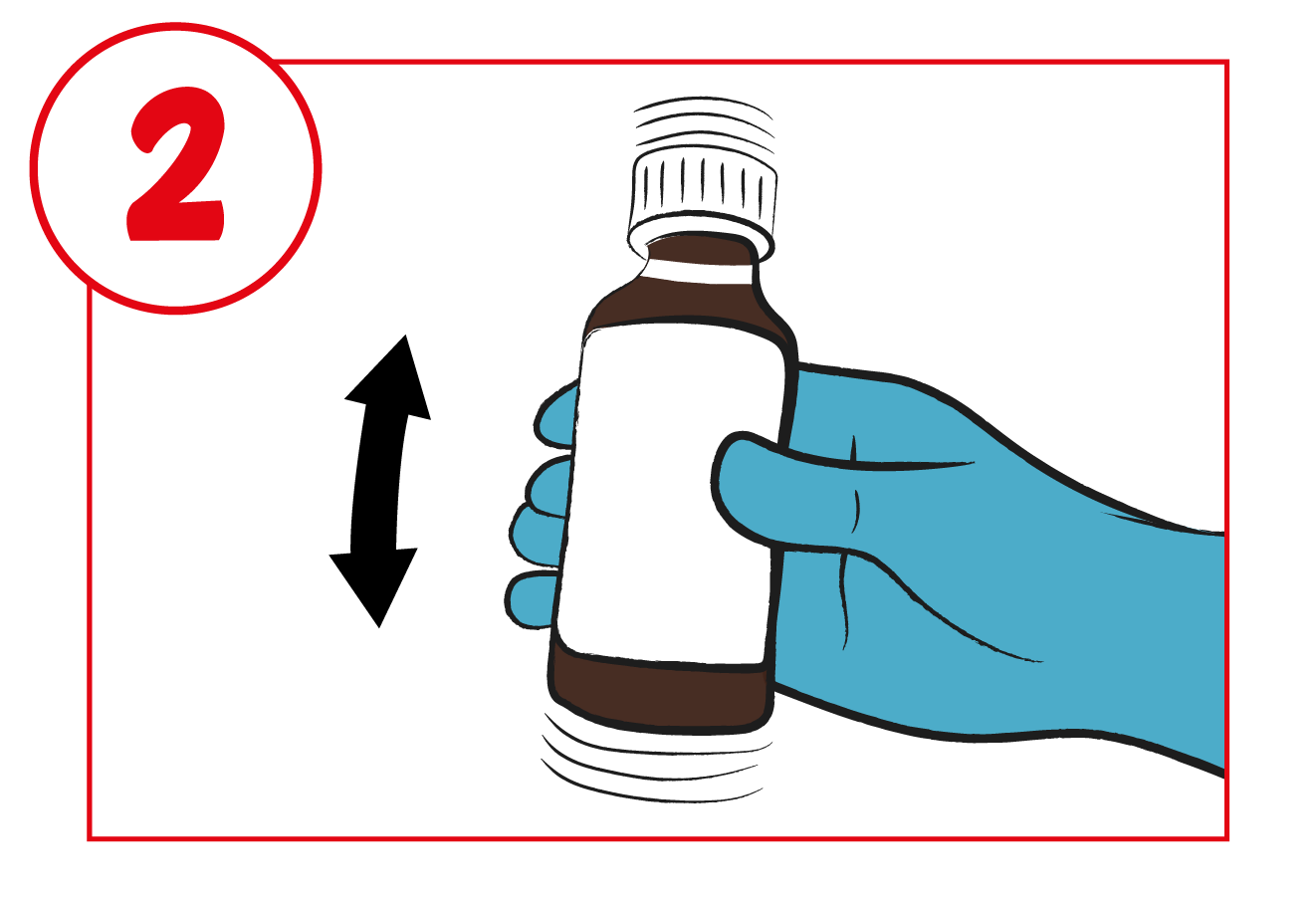
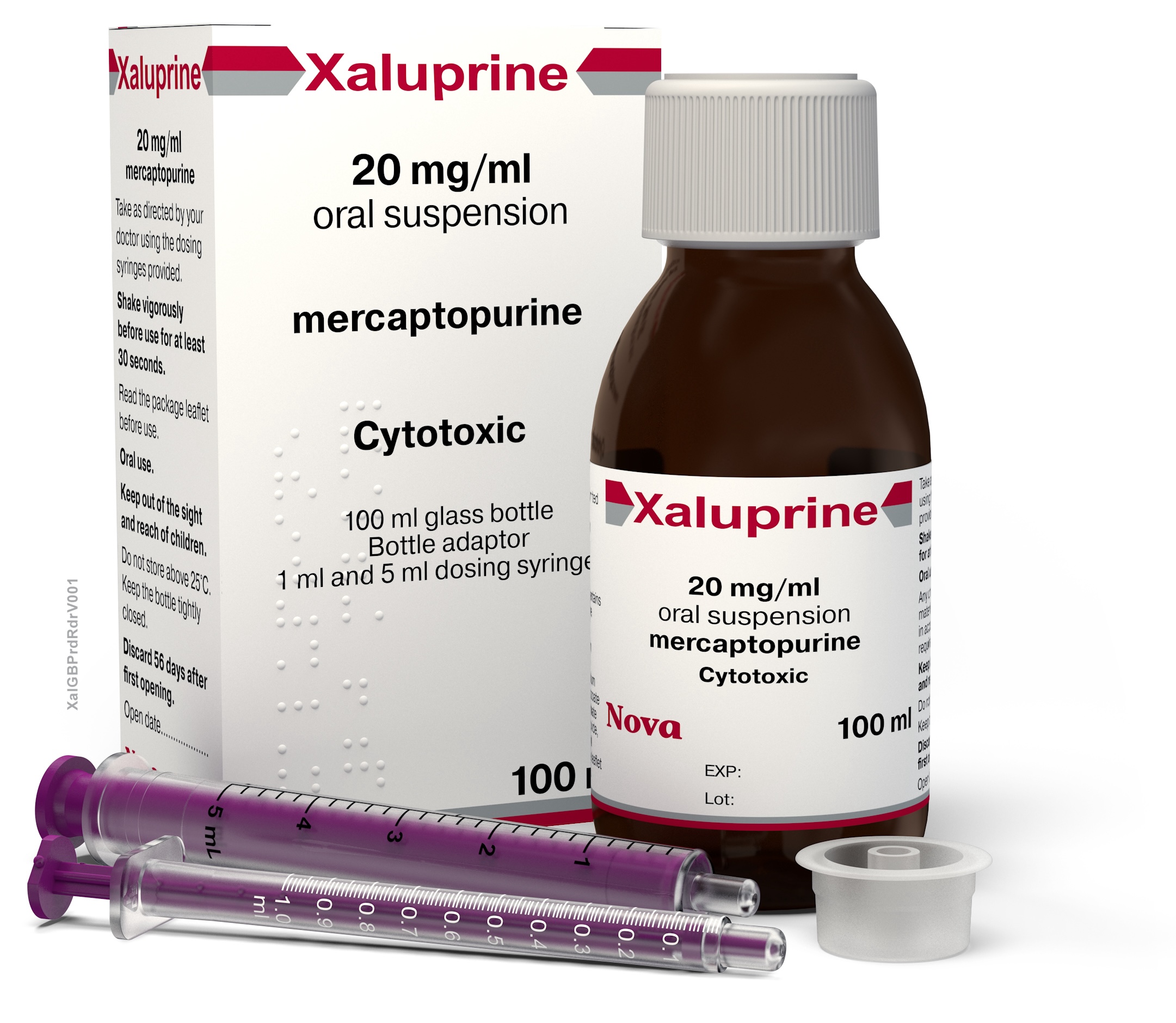
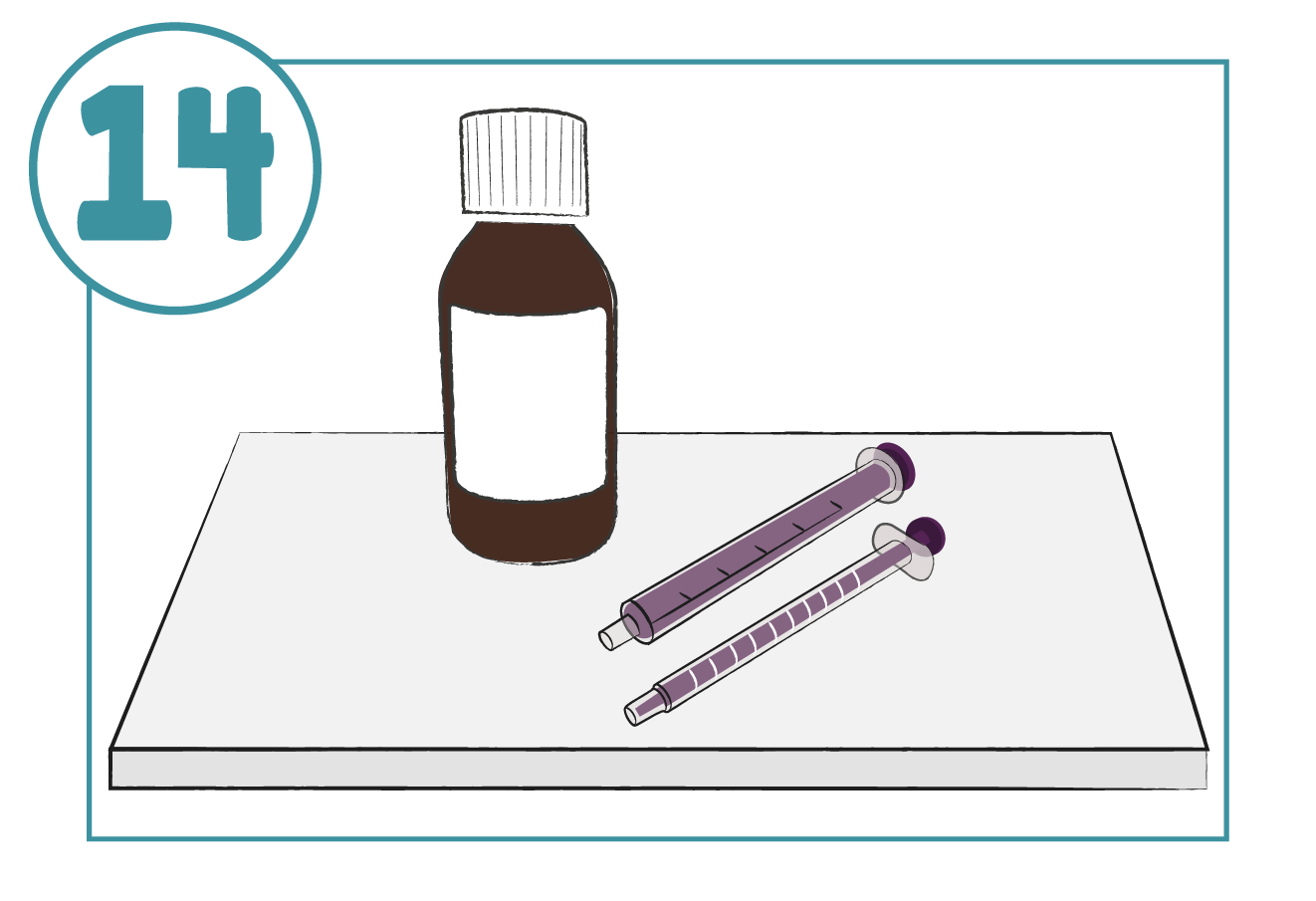
Shake the bottle vigorously for at least 30 seconds
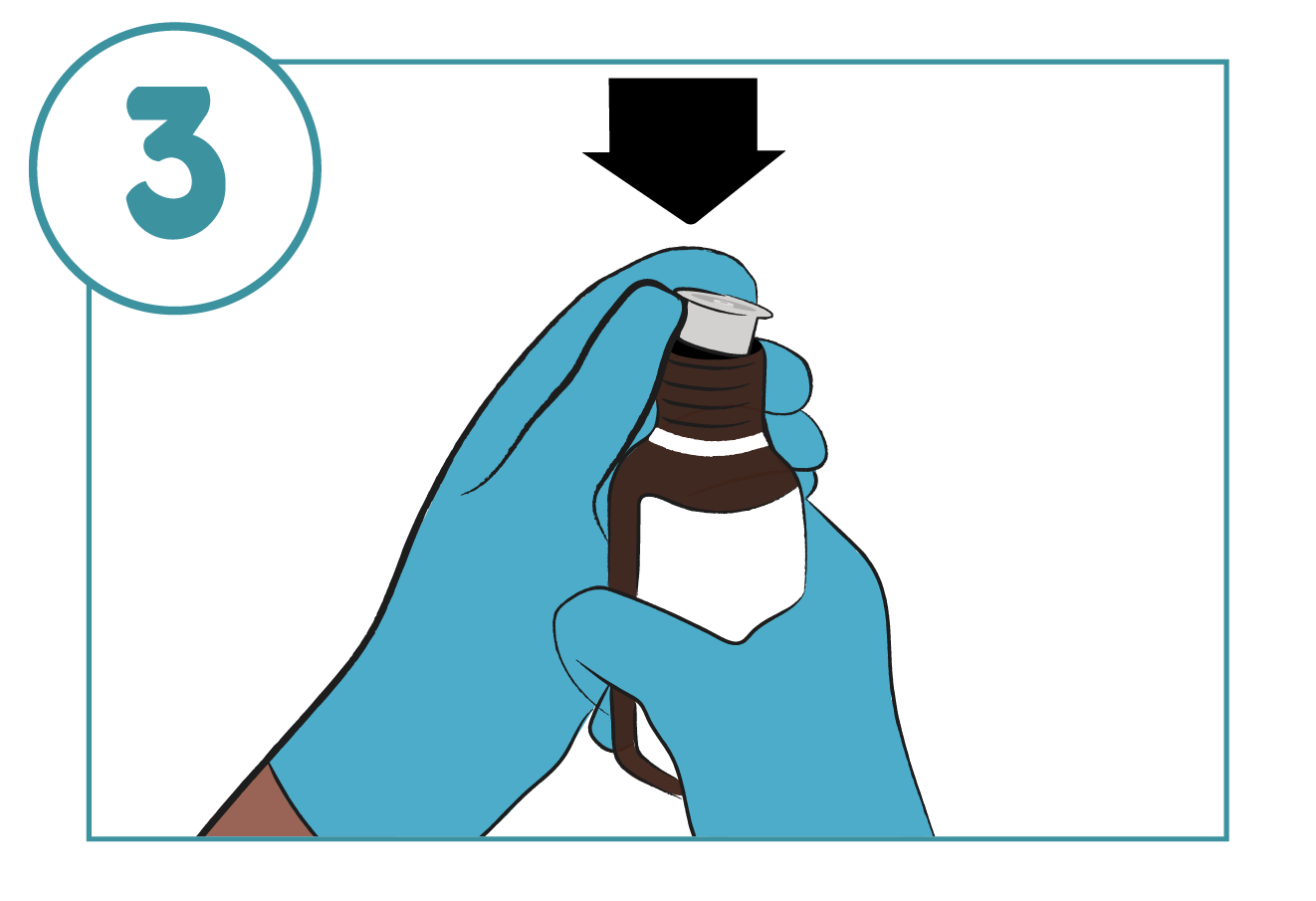
Remove the bottle cap and push the adaptor firmly into the top of the bottle. Leave in place for future doses
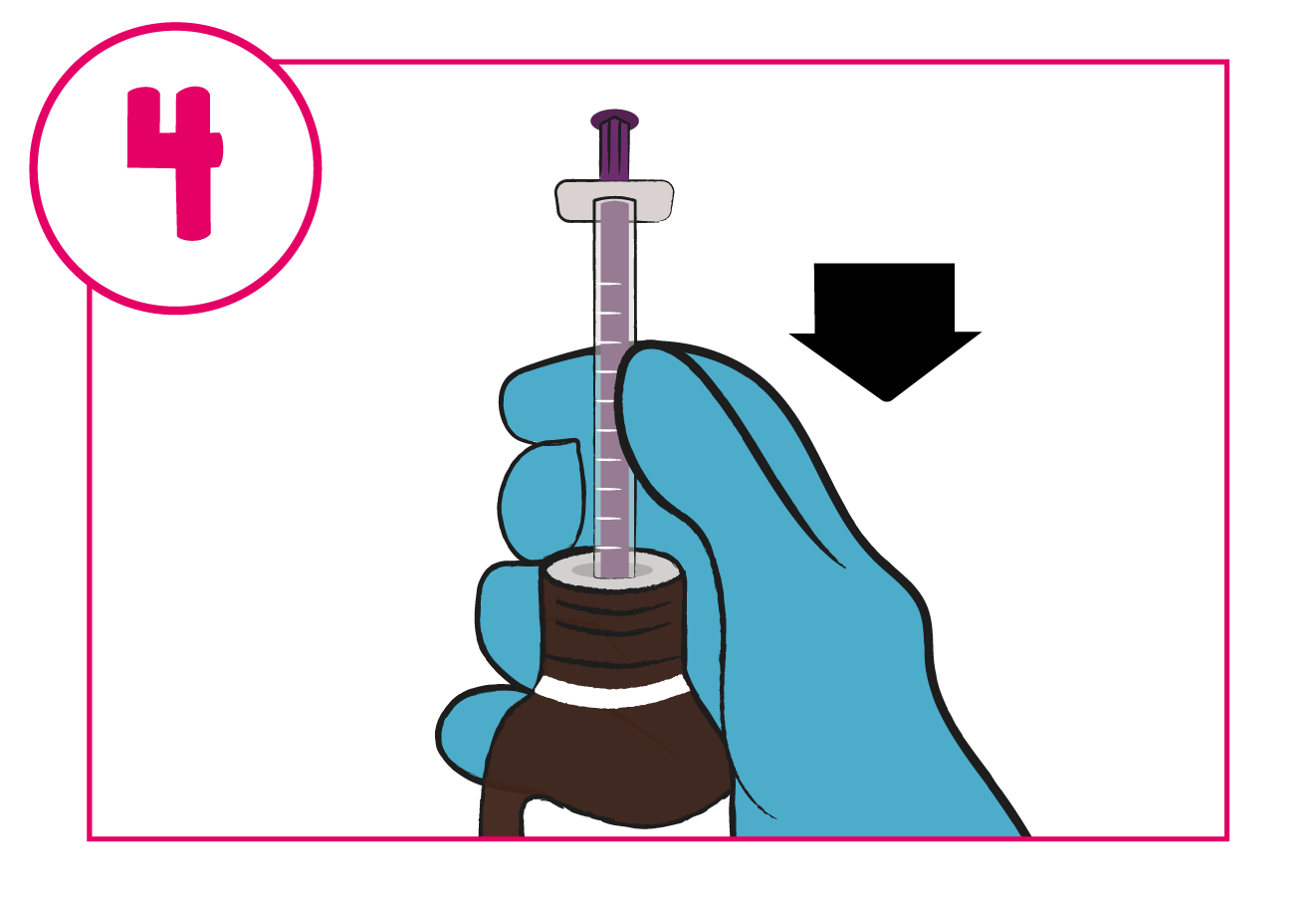
Push the tip of the dosing syringe into the hole in the adaptor
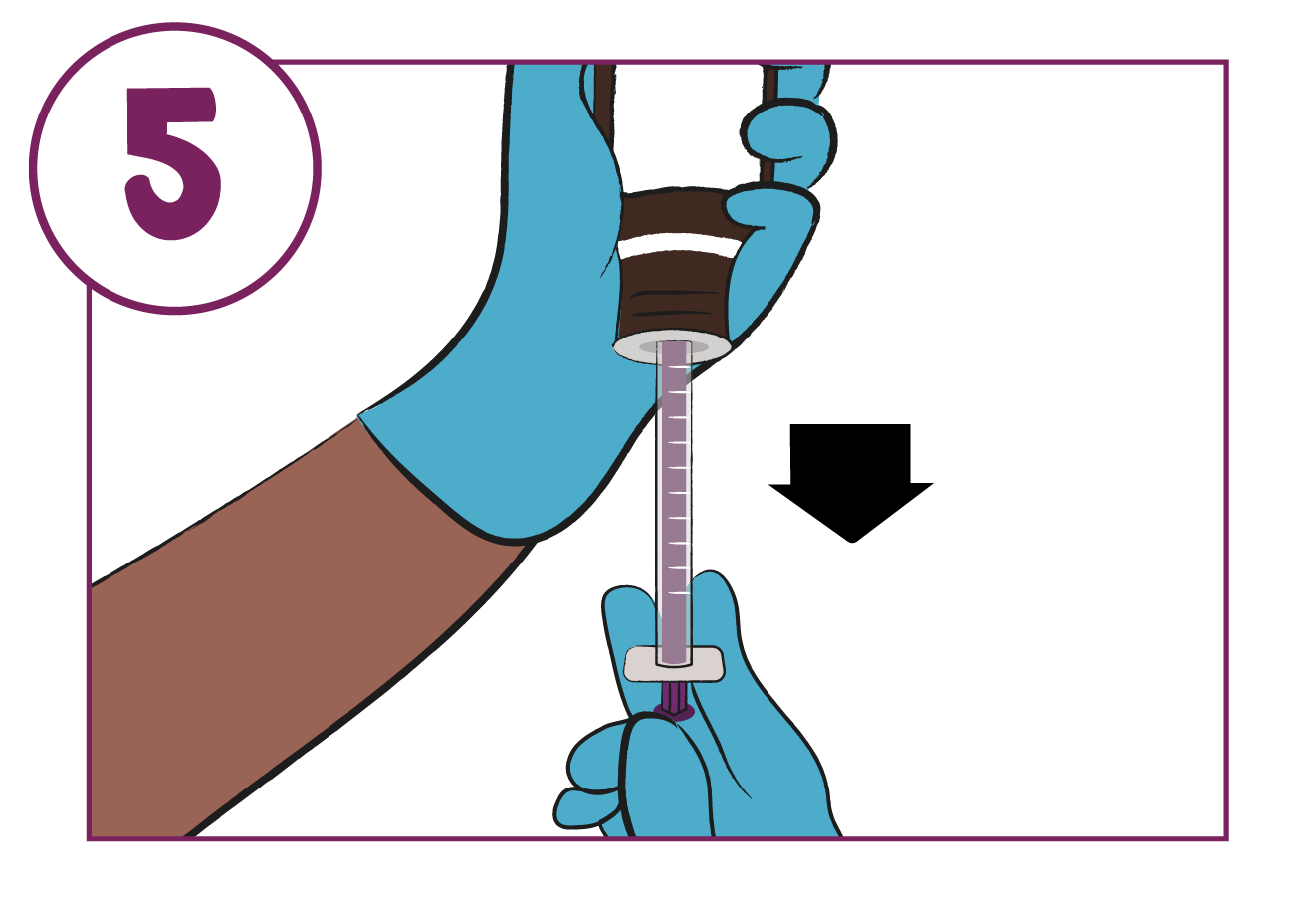
Turn the bottle upside down. Pull the plunger of the syringe back to the point on the scale that corresponds to the dose prescribed
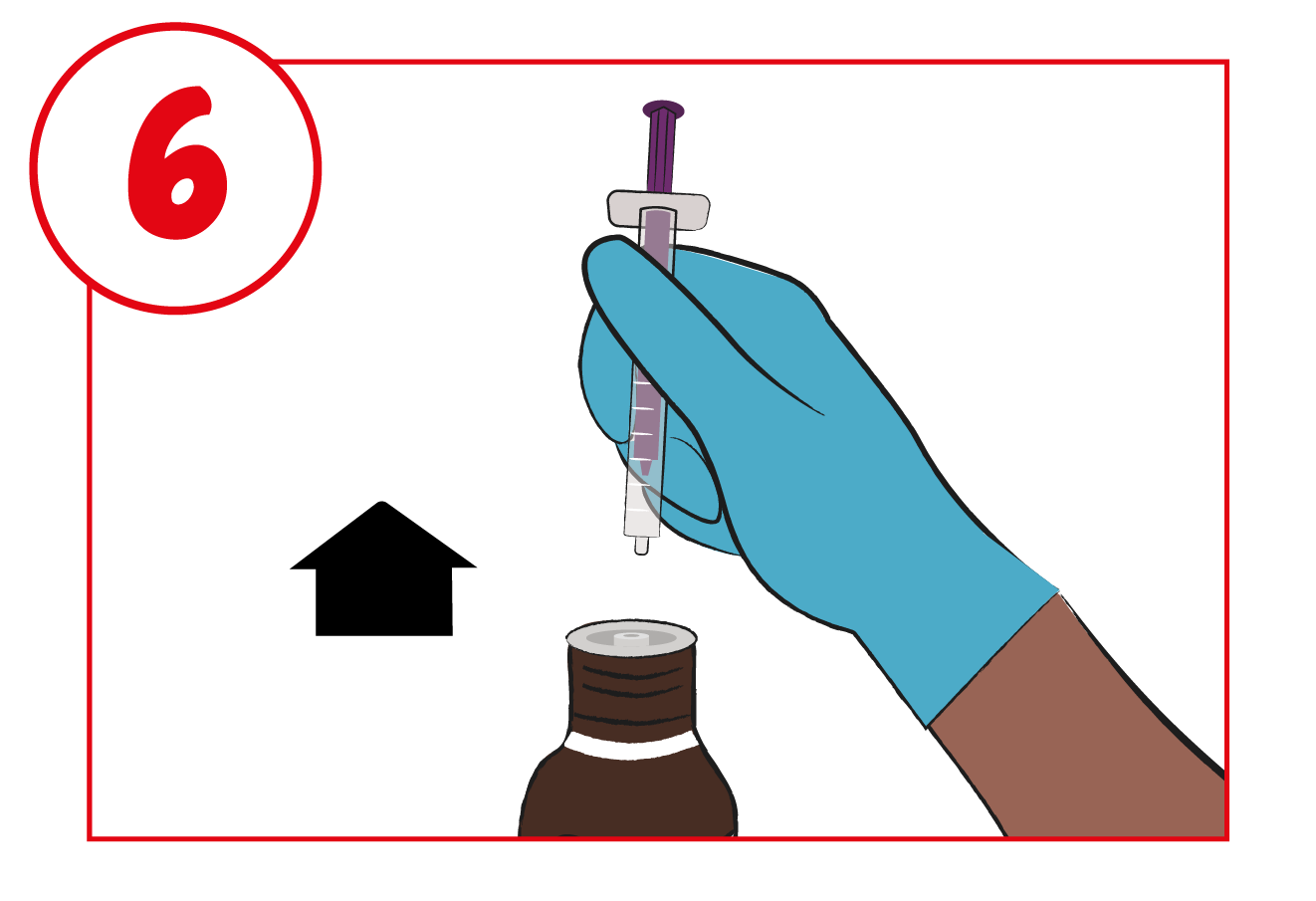
Turn the bottle back the right way up and carefully remove the syringe from the adaptor, holding it by the barrel rather than the plunger
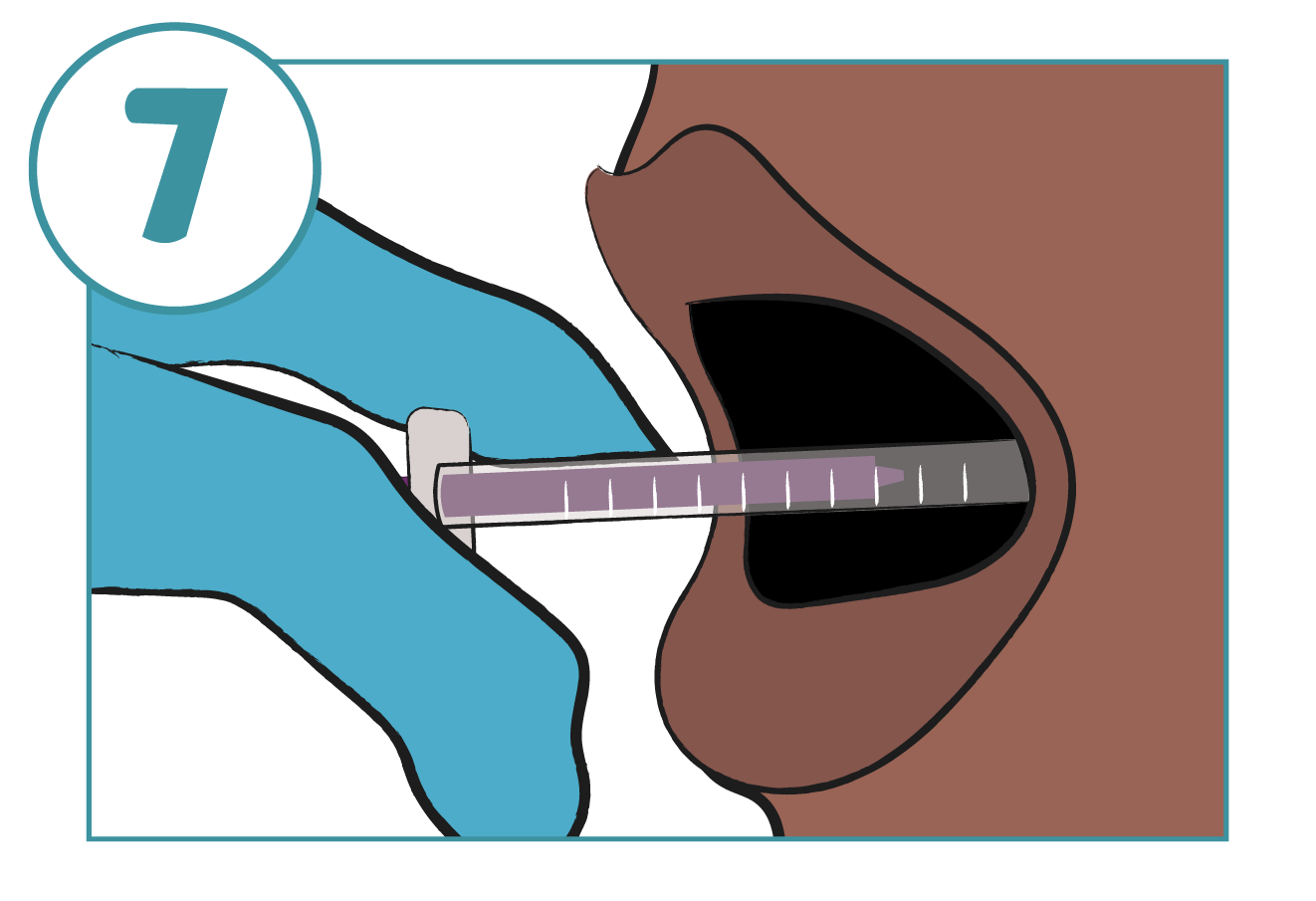
Gently put the tip of the syringe into your mouth and to the inside of your cheek
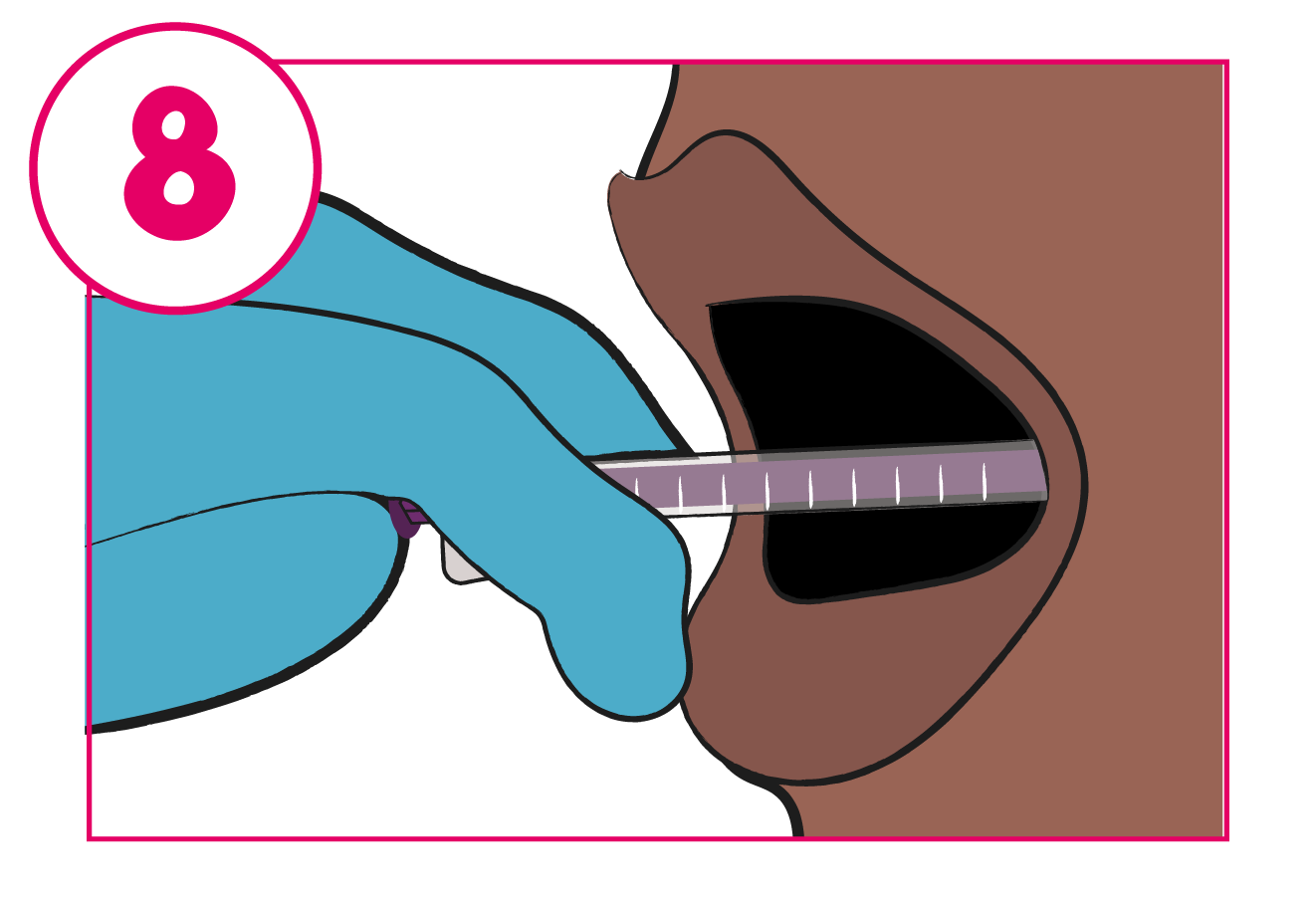
Slowly and gently push the plunger down to gently squirt the medicine into the inside of your cheek
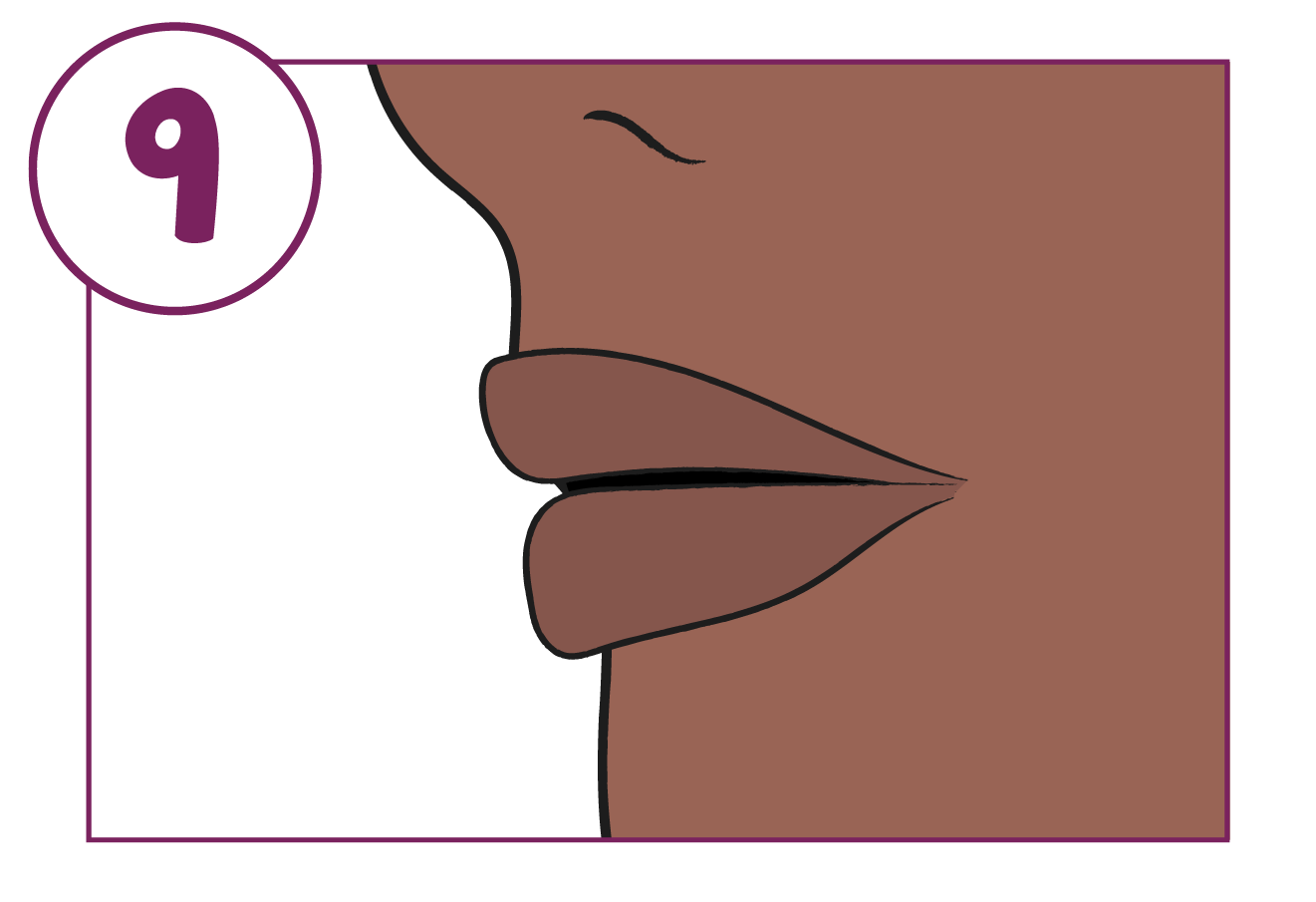
Remove the syringe from your mouth
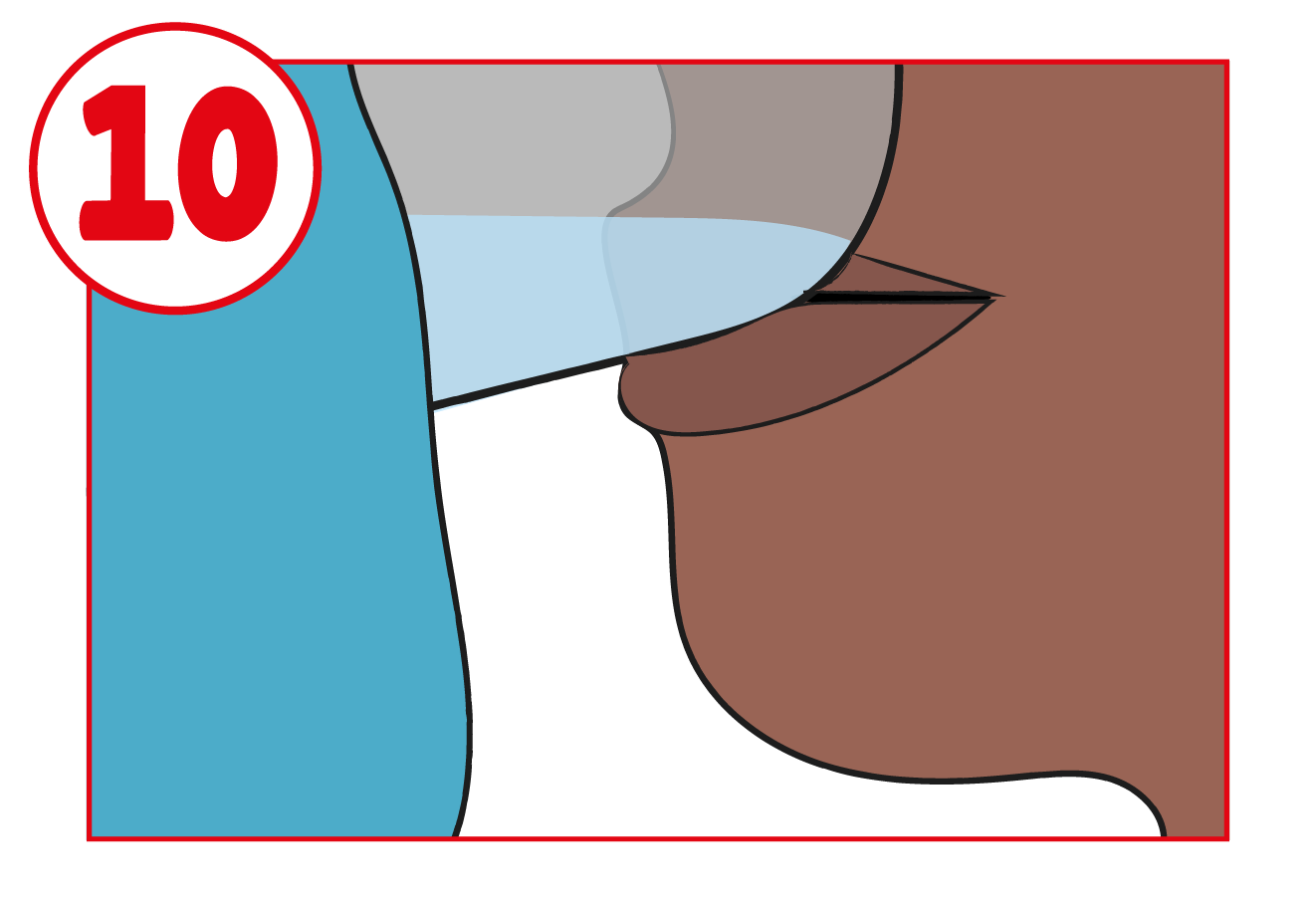
Swallow the medicine and drink some water, to ensure no medicine is left in your mouth
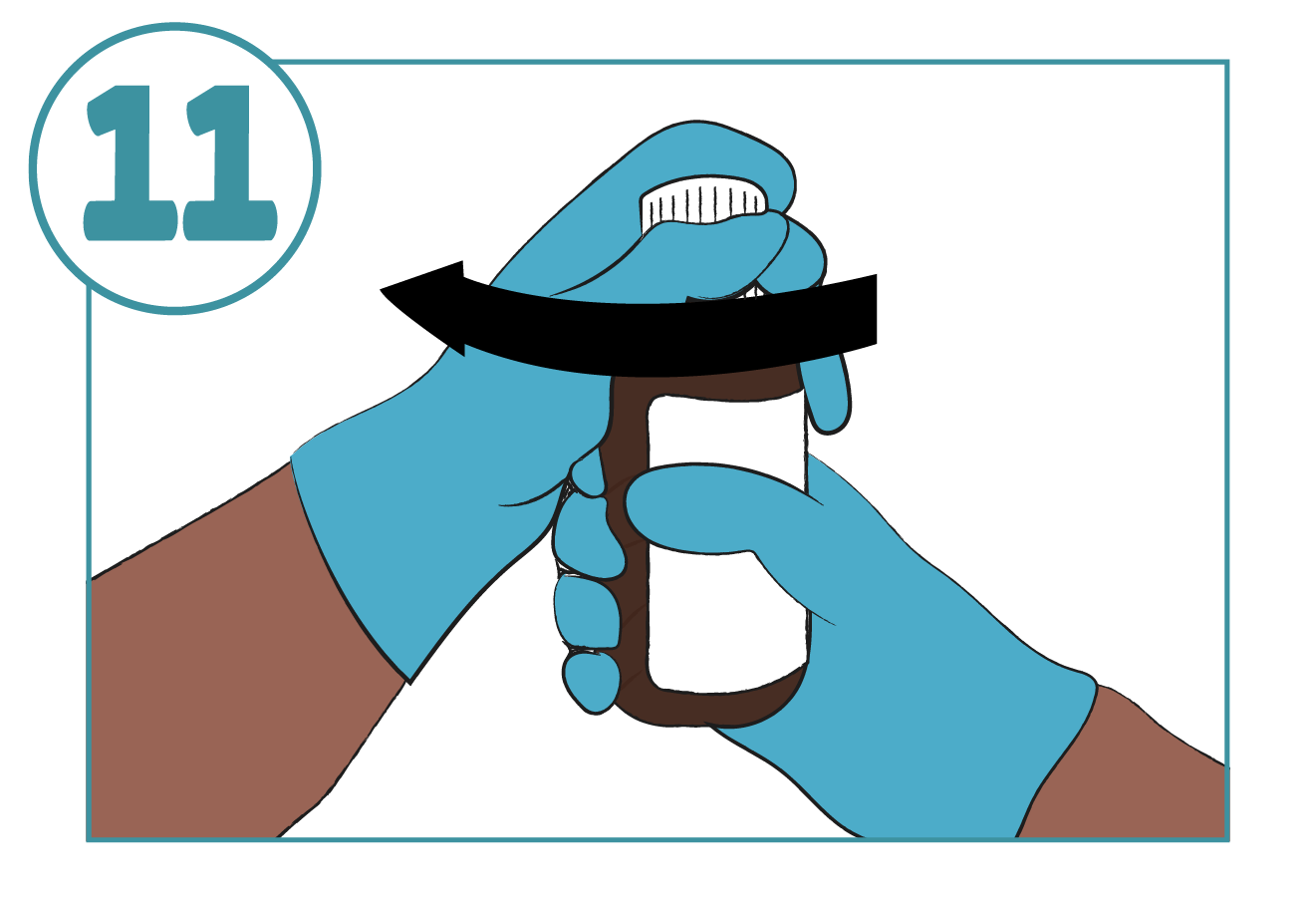
Put the cap back on the bottle with the adaptor left in place. Ensure that the cap is tightly closed

Wash the syringe with warm water and rinse well. Hold the syringe under water and move the plunger up and down several times to make sure the inside of the syringe is clean
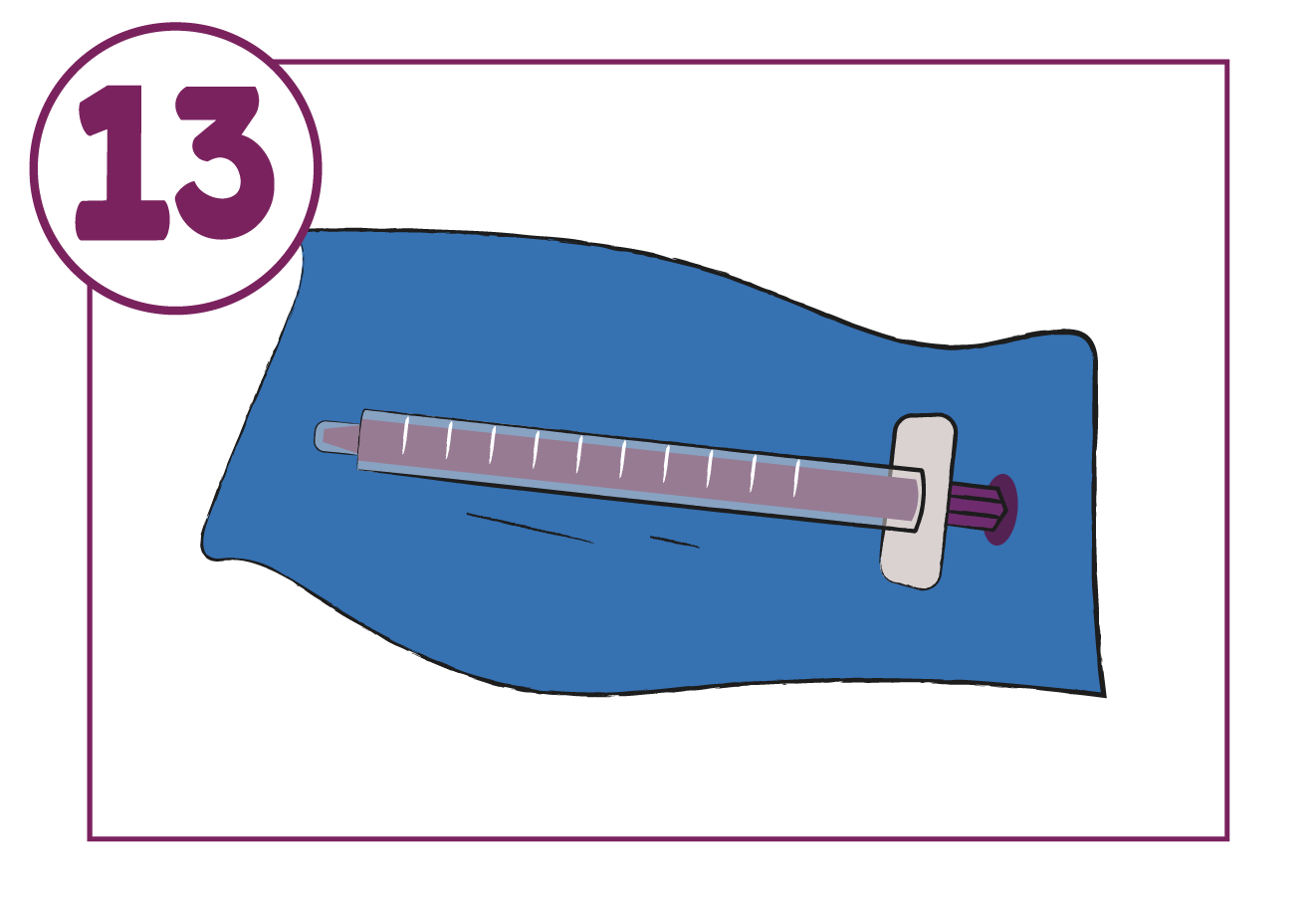
Let the syringe air-dry completely before you use it again
Store the syringe in a hygienic place with the medicine
View all Xaluprine® clinical information in one place
Downloads
These downloads (other than the HCP leaflet) are only for use with patients prescribed Xaluprine®.